

Mental health stigma remains one of the most persistent barriers to care, especially within religious communities where faith, culture, and social norms strongly shape perceptions of mental illness. Many individuals experience shame, fear of judgment, or the belief that seeking therapy reflects weak faith, all of which delay open conversations and treatment. Mental illness is frequently framed as a test of devotion or moral failing rather than a legitimate medical condition requiring professional intervention. Understanding how religious identity influences stigma and support is critical for developing culturally responsive approaches to care.
Methods: An anonymous Qualtrics survey was distributed from March to June 2025 across diverse religious communities in Ohio to assess perceived stigma, support, and attitudes toward professional mental health services. Recruitment occurred through campus email lists, word of mouth, QR codes in community spaces, and outreach at The Ohio State University, libraries, and gyms. Religious leaders further assisted by promoting the survey through bulletin boards and newsletters. The instrument included demographic items, Likert-scale statements, and limited open-ended questions designed to capture both quantitative and qualitative perspectives on mental health beliefs and barriers.
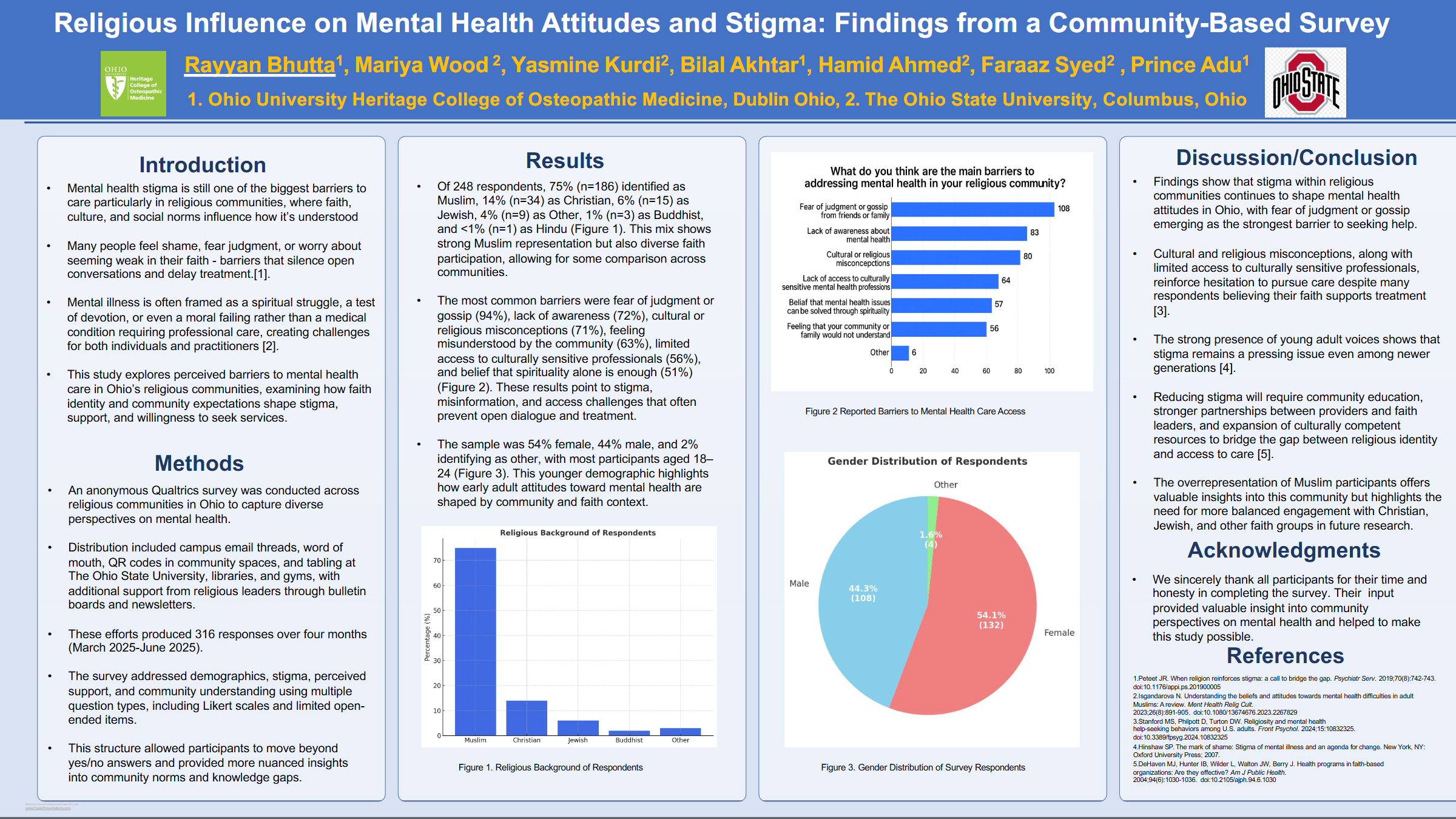
Results: A total of 316 responses were collected, of which 248 were complete and analyzable. Participants were 54% female, 44% male, and 2% identifying as other, with the majority aged 18–24. Most respondents identified as Muslim (75%), followed by Christian (14%), Jewish (6%), Other (4%), Buddhist (1%), and Hindu (<1%). The most frequently cited barriers to care were fear of judgment or gossip (94%), lack of awareness (72%), cultural or religious misconceptions (71%), feeling misunderstood by the community (63%), limited access to culturally sensitive professionals (56%), and belief that spirituality alone is sufficient (51%). These findings highlight stigma and misinformation as dominant obstacles, even among younger adults.
Conclusion: Stigma continues to shape mental health attitudes in Ohio’s religious communities. Despite widespread belief that faith supports seeking help, misconceptions and fear of judgment persist. Addressing these issues requires community education, stronger partnerships between providers and faith leaders, and expansion of culturally competent mental health resources to bridge the gap between religious identity and professional care.
UNDERLINE DOI: https://doi.org/10.48448/y7qd-pa56


